
For older adults, even a simple fall can result in a broken shoulder. These injuries are increasingly common, particularly in individuals with bones weakened by osteoporosis. Understanding the potential treatment for broken shoulder in elderly patients is helpful, as age-related factors often influence both healing and surgical decisions. In this post, we’ll examine how orthopedic specialists diagnose these fractures and outline the non-operative and operative strategies that guide treatment, helping patients and their families make informed decisions about recovery and care.
Key Takeaways
- Simple fractures may respond well to non-operative care, while complex, displaced fractures may necessitate surgical intervention.
- When surgery is required for complex, displaced fractures in older individuals, reverse shoulder replacement has emerged as a surgical option. It aims to provide pain relief and functional recovery.
- The treatment decision-making process should account for the patient’s pre-injury activity level, overall health, and specific functional expectations.
Understanding the Injury: Proximal Humerus Fractures
A proximal humerus fracture involves a break in the upper part of the humerus (the arm bone) near the shoulder joint. This area is a common site for fractures, particularly in older adults, due to the prevalence of osteoporosis, a condition that can reduce bone density and strength.
The vast majority of these fractures in the elderly result from a fall, typically from a standing height onto an outstretched hand or directly onto the shoulder. The force of the impact, transmitted up the arm to the weakened bone, causes the fracture.
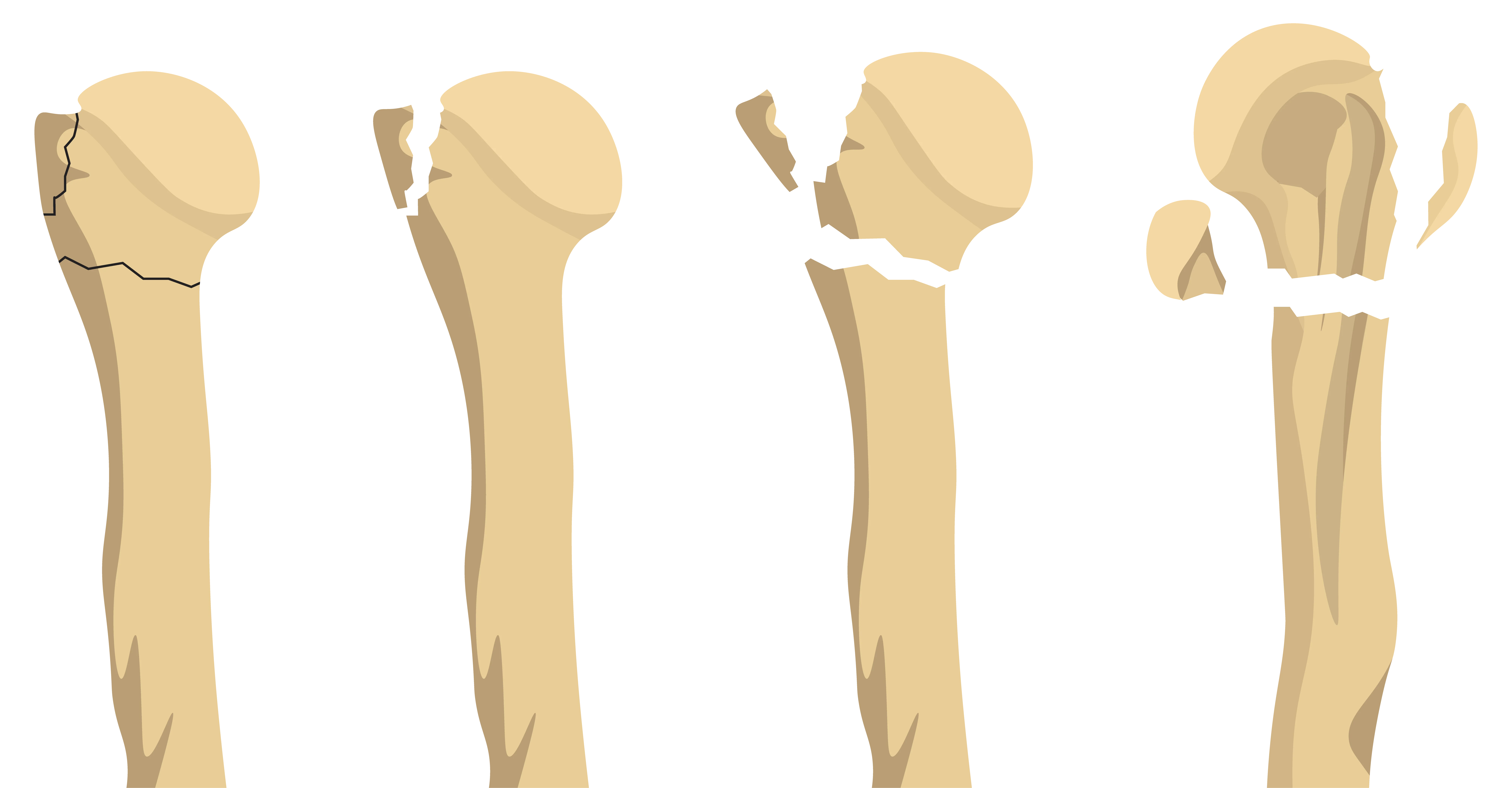
Classifying the Fracture
The most widely used classification method is the Neer system. It divides the proximal humerus into four segments, or “parts”: the articular head, the greater tuberosity, the lesser tuberosity, and the shaft. A fracture is classified by the number of displaced parts. The complexity of the fracture is a primary factor in determining whether non-operative or operative treatment is most appropriate.
Non-Operative Treatment: The First Line of Defense
For many elderly patients who sustain a proximal humerus fracture, non-operative management can be an effective treatment option.
The Goal of Non-Operative Care
The primary goal of non-operative treatment is to allow the fracture fragments to heal in a position that permits function. Non-operative treatment typically follows a structured, multi-phase protocol:
- Immobilization: The initial phase involves placing the arm in a sling or a specialized shoulder immobilizer. This can support pain control and help prevent further displacement of the fracture fragments.
- Early Passive Range of Motion (PROM): Once the initial pain subsides and the fracture shows early signs of stability, the patient may begin gentle, passive exercises. A physical therapist can assist the patient in moving the arm without the patient engaging their own muscles. This prevents the formation of scar tissue and joint stiffness.
- Active-Assisted and Active Range of Motion (AAROM/AROM): As healing progresses, the patient may start to use their own muscles to move the arm, initially with assistance and then independently. The focus shifts to restoring the full range of motion.
- Strengthening: The final phase, which can last for several months, frequently involves progressive resistance exercises to rebuild the strength of the rotator cuff and deltoid muscles.
Who May Benefit Most from Non-Operative Treatment?
- Minimally Displaced Fractures: Fractures where the fragments are well-aligned.
- Patients with Low Functional Demand: Individuals who are more sedentary or do not require a high level of overhead function.
- Patients with Comorbidities: Those for whom the risks of general anesthesia and surgery outweigh the potential benefits.
- Patients with Severe Osteoporosis: In cases of extremely poor bone quality, surgical fixation (using plates and screws) may fail to hold the fragments securely.
Operative Treatment: When Surgery Becomes Necessary
Certain fracture patterns and patient profiles can make surgical intervention a potential option. An experienced shoulder surgeon can evaluate the injury and help guide if surgery may be a recommended option for you. The decision is complex and depends on the degree of fracture displacement, the number of fragments, the patient’s bone quality, and their pre-injury activity level.
Indications for Surgery
Surgery may be considered for:
- Highly Displaced Fractures: Fractures where the fragments are significantly separated or angled, making functional healing unlikely.
- Fracture-Dislocations: Cases where the humeral head is fractured and also dislocated from the socket.
- Open Fractures: Fractures where the bone has broken through the skin.
- Active, High-Demand Patients: Individuals who are very active and have a high functional expectation for their shoulder.
Surgical Options for Broken Shoulder in Elderly
Open Reduction and Internal Fixation (ORIF): In this procedure, the surgeon opens the shoulder, realigns the bone fragments (open reduction), and secures them with a plate and screws (internal fixation).
Reverse Total Shoulder Arthroplasty: In a reverse shoulder replacement, the anatomy of the shoulder is “reversed”: a metal ball (glenosphere) is fixed to the shoulder socket (glenoid), and a plastic socket is placed on the top of the arm bone (humerus). The reverse design shifts the center of rotation, enabling the deltoid muscle to lift the arm even if the rotator cuff tendons are damaged.
The Importance of Rehabilitation
The success of the treatment for broken shoulder in elderly may depend on a dedicated and structured rehabilitation program. The primary goals of the rehabilitation process are pain management, restoration of range of motion, strengthening, and supporting a return to daily activities.
A physical therapist is frequently a key partner in recovery. They can design a personalized program based on the patient’s specific fracture pattern, the type of treatment received, and the patient’s progress.
Conclusion
Treating a broken shoulder in older individuals is a highly individualized process that demands careful consideration of the fracture pattern, the patient’s bone quality, and their overall health. By working closely with a dedicated shoulder specialist and committing fully to the rehabilitation process, elderly patients can pursue a path toward recovery.
Frequently Asked Questions
Is surgery always necessary for a broken shoulder in the elderly?
Not always. Many proximal humerus fractures in the elderly are treated successfully without surgery. Non-operative treatment can be the preferred approach for stable, minimally displaced fractures. Surgery may be reserved for complex, highly displaced fractures, fracture-dislocations, or for active patients with high functional demands where non-operative treatment is unlikely to restore adequate function.
What is the difference between a total shoulder replacement and a reverse total shoulder replacement for a fracture?
A total shoulder replacement replaces the ball and socket with prosthetic components that mimic the natural anatomy. It generally relies on a healthy, functioning rotator cuff. A reverse shoulder replacement reverses the ball and socket position. This design allows the deltoid muscle to power the arm’s movement, bypassing the need for a functional rotator cuff.
How long does it take for a broken shoulder to heal in the elderly?
Healing time varies based on the fracture’s severity and the patient’s overall health. Many proximal humerus fractures take around 3 months to heal. Full functional recovery, especially with physical therapy, may take longer. Surgical patients often follow a structured rehabilitation program that extends 4 to 6 months.
